
Epicondylitis is a condition many tennis players and golfers will be familiar with. The repetitive movements associated with these activities can lead to pain in the lateral and medial tendons attached to the elbow, resulting in the conditions known commonly as ‘tennis elbow’ and ‘golfer’s elbow.’1
Tennis elbow is the most common cause of elbow pain, with 1-3% of adults affected every year, and a higher incidence in those aged 40-60.2 If untreated, the condition can continue for an average of 6-24 months.3
One type of non-surgical treatment for epicondylitis is bracing, but how effective is it? This article looks at the clinical evidence for forearm orthoses, and introduces a new elbow brace from DonJoy®, EpiForce® Strong.
What is epicondylitis?
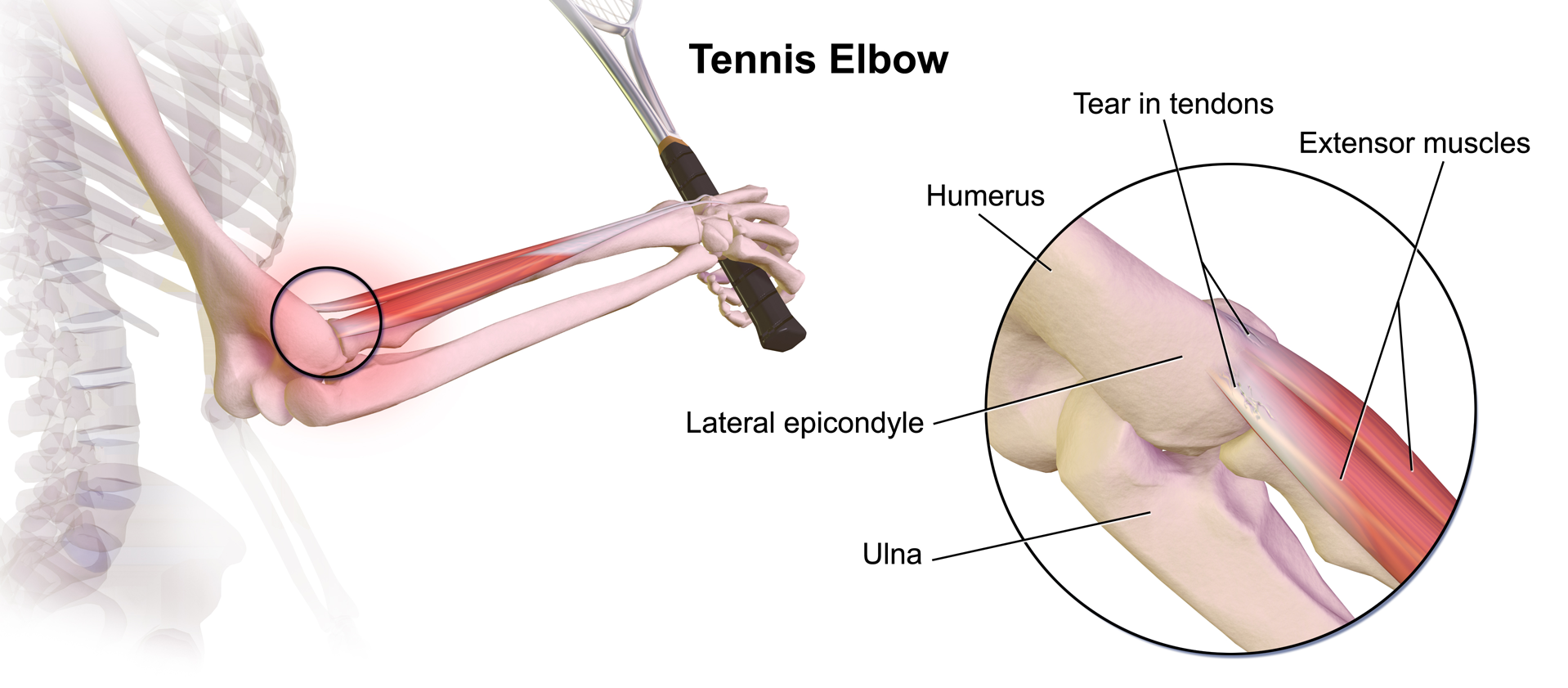
Epicondylitis is clinically defined as pain in the region of the epicondyle (a rounded protuberance at the end of a bone).1 The pain is often caused by inflammation or micro-tearing of the tendons that join the forearm muscles on the elbow.3
• Lateral epicondylitis: Pain in the tendons that attach on the outside of the elbow. Also known as tennis elbow
• Medial epicondylitis: Pain in the tendons that attach on the inside of the elbow. Also known as golfer’s elbow
What causes epicondylitis?
The overuse aspect of epicondylitis is often caused by repetitive wrist extension with alternating supination/pronation, hence its association with tennis and golf.3
However, these injuries can also be caused by forceful or repetitive work tasks, such as those involving non-neutral positions of the upper extremities, use of heavy tools, and high physical strain.4 Obesity and smoking are also risk factors for medial epicondylitis.1
Treatment of epicondylitis
Epicondylitis is first treated non-operatively, with a reported success rate of 90% over 12 to 18 months.5 Surgery is usually only recommended when conservative management fails to relieve symptoms after 6 to 12 months.6
Types of non-surgical epicondylitis treatment include:
- Counterforce bracing
- NSAIDs
- Physical therapy and activity modification
- Corticosteroid injections
- Shockwave therapy
These interventions are aimed at relieving tendon strain, reducing tendon irritation and inflammation, and allowing the tendons to heal.5
Elbow bracing for epicondylitis
Elbow counterforce bracing is prescribed in 77% of tennis elbow (lateral epicondylitis) cases in the USA.2 The most common type is a forearm orthosis, a band worn around the forearm to reduce loading on the extensor tendons of the elbow.
However, because the way in which these braces reduce pain and improve function in elbow epicondylitis is not well understood, it may be helpful to review a selection of clinical studies.7
Kroslak et al.’s 2019 clinical trial found that wearing Procare elbow braces reduced the level and frequency of pain for patients suffering lateral epicondylitis. They also helped reduce difficulties with picking up objects and twisting motions, lateral epicondyle tenderness, grip strength, and overall elbow function. Of the two braces used, the padded counterforce brace appeared to accelerate the recovery process and provide better pain relief.8

In their 2019 study, Barati et al. found that both an elbow band and an elbow sleeve were effective in improving proprioception, pain severity, and force production in the hand. However, better finger dexterity was achieved with the forearm band only.9
In their study comparing an elbow band to a wrist orthosis for treating epicondylitis, Akkurt et al. (2018) found both were effective. Pain, function, muscle strength, and quality of life were all improved.10
The results of Sadeghi-Demneh et al.’s 2013 study showed an elbow band and sleeve and a wrist brace all provided immediate improvement in lateral epicondylitis pain severity. Overall, the elbow band and sleeve were more effective.11
Heales et al.’s 2020 systematic review found that forearm orthoses can immediately reduce pain during contraction and improve pain-free grip strength, but not maximal grip strength, in individuals with lateral elbow tendinopathy.7
In conclusion, the literature presented here shows elbow bracing reduces frequency and level of pain, and improves function, pain-free grip strength, proprioception, and finger dexterity for patients with elbow epicondylitis.
Introducing EpiForce® Strong from DonJoy® – the easy way to elbow relief
When it comes to pain relief for the elbow, EpiForce Strong is the easy option.
Thanks to its removable pressure pad, DonJoy’s latest product offers a 2-in-1 bracing solution for tennis and golfer’s elbow. By simply moving the pad to the appropriate position, the brace can be used to help provide targeted pain relief for either lateral or medial epicondylitis.
Fitting is fast and simple and can be achieved with just one hand. Made from snap-fit material, the support wraps instantly around the arm and stays there while the patient clips the buckle into place. The single strap can then be adjusted easily to provide the suitable degree of compression; tighten the strap during activity, loosen it during periods of rest.

Lightweight and low profile, the brace can be worn comfortably throughout the day. And with universal sizing for either arm, EpiForce Strong even takes the hassle out of ordering.
References
- Shiri, R., Viikari-Juntura, E., Varonen, H. and Heliövaara, M., 2006. Prevalence and determinants of lateral and medial epicondylitis: a population study. American journal of epidemiology, 164(11), pp.1065-1074.
- Sanders Jr, T.L., Maradit Kremers, H., Bryan, A.J., Ransom, J.E., Smith, J. and Morrey, B.F., 2015. The epidemiology and health care burden of tennis elbow: a population-based study. The American journal of sports medicine, 43(5), pp.1066-1071.
- Johnson, G.W., Cadwallader, K., Scheffel, S.B. and Epperly, T.D., 2007. Treatment of lateral epicondylitis. American family physician, 76(6), pp.843-848.
- Haahr, J.P. and Andersen, J.H., 2003. Physical and psychosocial risk factors for lateral epicondylitis: a population based case-referent study. Occupational and environmental medicine, 60(5), pp.322-329.
- Ahmed, A.F., Rayyan, R., Zikria, B.A. and Salameh, M., 2022. Lateral epicondylitis of the elbow: an up-to-date review of management. European Journal of Orthopaedic Surgery & Traumatology, pp.1-6.
- Calfee, R.P., Patel, A., DaSilva, M.F. and Akelman, E., 2008. Management of lateral epicondylitis: current concepts. JAAOS-Journal of the American Academy of Orthopaedic Surgeons, 16(1), pp.19-29.
- Heales, L.J., McClintock, S.R., Maynard, S., Lems, C.J., Rose, J.A., Hill, C., Kean, C.O. and Obst, S., 2020. Evaluating the immediate effect of forearm and wrist orthoses on pain and function in individuals with lateral elbow tendinopathy: a systematic review. Musculoskeletal Science and Practice, 47, p.102-147.
- Kroslak, M., Pirapakaran, K., & Murrell, G. (2019). Counterforce bracing of lateral epicondylitis: a prospective, randomized, double-blinded, placebo-controlled clinical trial. Journal of shoulder and elbow surgery, 28(2), 288–295.
- Barati, H., Zarezadeh, A., MacDermid, J. C., & Sadeghi-Demneh, E. (2019). The immediate sensorimotor effects of elbow orthoses in patients with lateral elbow tendinopathy: a prospective crossover study. Journal of shoulder and elbow surgery, 28(1), e10–e17.
- Akkurt, H. E., Kocabaş, H., Yılmaz, H., Eser, C., Şen, Z., Erol, K., G ksu, H., Karaca, G., & Baktık, S. (2018). Comparison of an epicondylitis bandage with a wrist orthosis in patients with lateral epicondylitis. Prosthetics and orthotics international, 42(6), 599–605.
- Sadeghi-Demneh, E., & Jafarian, F. (2013). The immediate effects of orthoses on pain in people with lateral epicondylalgia. Pain research and treatment, 2013, 353597.







