Ask anyone who has rolled their ankle during sport whether they should be wearing a brace, and you’ll likely get one of two answers: “Absolutely — I wear one every time I play” or “No, I need to strengthen it without one.” Both responses reflect common but incomplete ideas about what ankle bracing is actually for. This article details the recommended use of ankle bracing and how it can affect sprain rehabilitation.
Misconceptions Around Ankle Bracing
One of the most persistent misconceptions about ankle bracing is that wearing one weakens the ankle or creates long-term dependency. This concern often leads people to stop using the brace too soon, exposing healing tissues to loads they’re not yet ready to handle.
Current evidence around ankle bracing does not support this assumption. Used strategically, an ankle brace can be a tool that enables rehabilitation to progress more safely and confidently.1,2,3
What an Ankle Brace Actually Does
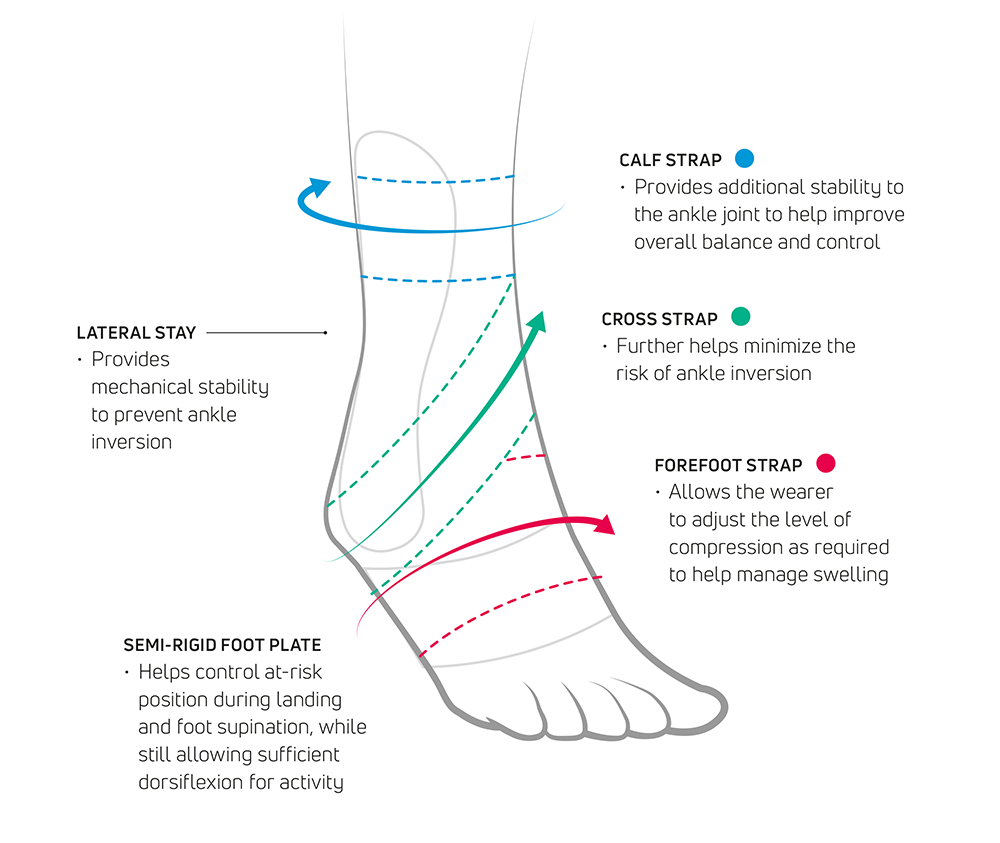
Depending on the design, an ankle brace can contribute to rehabilitation in several important ways:
- Improving mechanical stability around the joint1
- Reducing excessive range of motion during dynamic activity2
- Enhancing proprioceptive input — the body’s sense of position and movement3
- Supporting neuromuscular control1
- Improving the individual’s sense of contact and control through the foot and ankle3
Following an ankle sprain, tissues may regain their range of motion and basic strength before they have fully adapted to the demands of running, cutting, and dynamic loading. During this transitional period, a brace can provide an appropriate level of external support that allows individuals to progress rehabilitation tasks with confidence, without exposing the ankle to excessive stress.
Matching the Brace to the Injury and Stage of Recovery
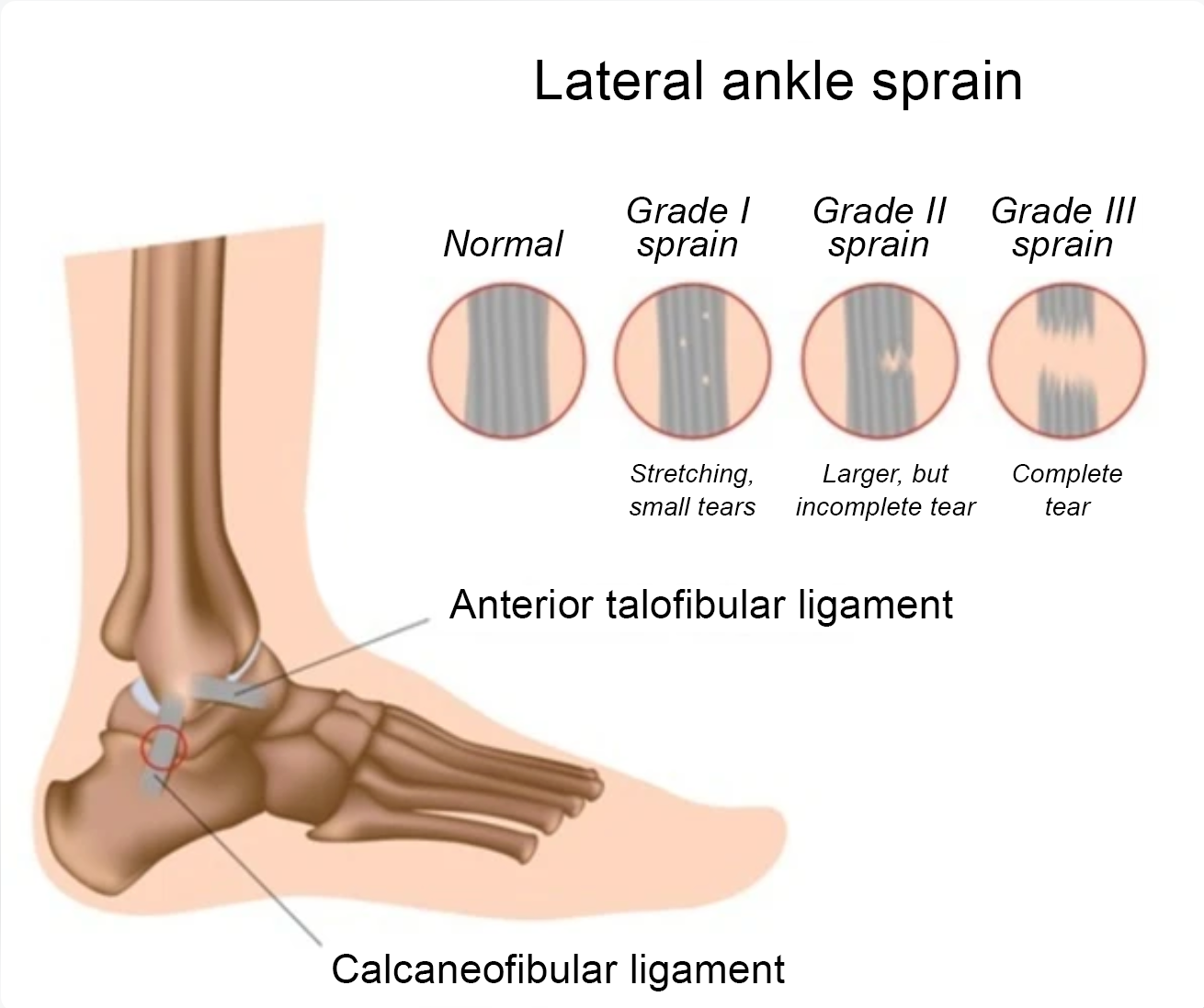
Ankle sprains are graded by severity — from a Grade I (mild stretching of the ligament fibres) through to a Grade III (complete ligament tear with significant instability) — and the appropriate level of external support should reflect this.

Milder sprains typically benefit from lightweight or elastic supports. These provide compression and proprioceptive feedback without limiting movement excessively, helping to maintain sensorimotor awareness while preserving a high degree of mobility.3
Moderate to more severe sprains may require semi-rigid or stabilizing braces that offer greater mechanical support during weight-bearing and dynamic activity. These designs can help improve ankle stiffness, reduce excessive range of motion, and provide additional stability while the individual progresses through rehabilitation.1,2,4
Bracing needs also change as recovery progresses. Early in rehabilitation, the primary goal is to protect healing structures and manage swelling. As recovery advances, the focus shifts toward controlled loading, proprioceptive development, and sport-specific demands. For those returning to running or field-based sports, bracing may be used temporarily during higher-risk activities while strength, neuromuscular control, and confidence continue to develop.
How Ankle Braces Affect Confidence
Rather than being simply a physical process, psychological readiness plays a significant role in successful recovery from an ankle sprain. Even when physical measures have improved, apprehension around injury recurrence can influence movement strategies and loading behavior — often in ways that create new problems elsewhere in the kinetic chain.
This is where ankle bracing can make a particularly valuable contribution. By providing a sense of stability during early return to running or sport-specific drills, and allowing graded exposure to higher-risk movements such as cutting or uneven terrain, a brace can help an individual move more naturally, reducing the hesitant or protective patterns that often persist long after the physical injury has resolved.
What the Research Shows
Clinical evidence supports the strategic use of bracing in ankle rehabilitation. Studies have shown that bracing may reduce talar tilt and slow simulated sprain motion in unstable ankles, improve performance in functional tasks such as shuttle running, and enhance dynamic balance in people with functional ankle instability.2,5,6,7
A randomized controlled trial involving athletes with a history of lateral ankle sprain found that bracing was more effective than neuromuscular training alone in preventing recurrence.8 A subsequent systematic review concluded that the body of available research strongly supports the positive effect of ankle braces on dynamic balance in those with chronic ankle instability.9
Summary
Ankle bracing, used thoughtfully and matched to the individual’s injury severity, rehabilitation stage, and activity demands, is a clinically supported strategy that protects healing tissue, builds movement confidence, and enables rehabilitation to progress effectively.
Different stages of recovery often require different levels of support. The following brace options illustrate how support can be matched to injury severity and rehabilitation goals.
Ankle Bracing from Enovis™ — A Brace for Every Sprain
Under the Aircast® and DonJoy® brands, the Enovis™ portfolio of ankle braces offers a comprehensive choice of treatment options for all severities of ankle sprain, as well as chronic instability.
Grade I



DonJoy StrapiLax™ Ankle
DonJoy FusioLight II®
Aircast AirSport™
DonJoy StrapiLax™ Ankle — Elastic knitted ankle support with malleolar pads and adjustable strapping
DonJoy FusioLight II® — Semi-rigid ankle stirrup with memory-foam inserts
Aircast AirSport™ — Semi-rigid ankle support with foam-filled aircell
Grade II



Aircast Air-Stirrup™
Aircast AirSport+®
Aircast ActyFoot™
Aircast Air-Stirrup — Semi-rigid ankle stirrup with aircells for edema management
Aircast AirSport+ — Semi-rigid ankle support with BOA®* dial for adjustable compression
Aircast ActyFoot — Semi-rigid ankle support with modular design
Grade III


Aircast AirSelect™ Elite
Aircast AirSelect™ Standard
Aircast AirSelect Elite — Premium full-shell walking boot with adjustable edema control
Aircast AirSelect Standard — Full-shell walking boot with adjustable aircells
Chronic Ankle Instability


DonJoy ActyLight®
Aircast A60™
Aircast AirSport™
Aircast ActyFoot™
DonJoy ActyLight — Semi-rigid ankle support with step-in design
Aircast A60 — Semi-rigid ankle support with stabilizer
Aircast AirSport™
Aircast ActyFoot
For more information about managing ankle sprains and finding the right support, visit our website.
Healthcare professionals interested in learning more about ankle braces can contact their local Enovis representative or visit our website for detailed product information.
BOA® is a registered trademark of Boa Technology, Inc.
References
- Zhang G, Zha C, Cao S, Xiong L, Huang P, Zhang G, Ji Y. Effect of a semirigid ankle brace on the in vivo kinematics and muscle activity of patients with functional ankle instability during simulated ankle sprain. Medicine (Baltimore). 2024 Aug 9;103(32):e37832.
- Tang YM, Wu ZH, Liao WH, Chan KM. A study of semi-rigid support on ankle supination sprain kinematics. Scand J Med Sci Sports. 2010 Dec;20(6):822-6.
- Forbes H, Thrussell S, Haycock N, Lohkamp M, White M. The effect of prophylactic ankle support during simulated soccer activity. J Sport Rehabil. 2013 Aug;22(3):170-6.
- Zinder SM, Granata KP, Shultz SJ, Gansneder BM. Ankle bracing and the neuromuscular factors influencing joint stiffness. J Athl Train. 2009 Jul-Aug;44(4):363-9.
- Vaes PH, Duquet W, Casteleyn PP, Handelberg F, Opdecam P. Static and dynamic roentgenographic analysis of ankle stability in braced and nonbraced stable and functionally unstable ankles. Am J Sports Med. 1998 Sep-Oct;26(5):692-702.
- Crockett NJ, Sandrey MA. Effect of Prophylactic Ankle-Brace Use During a High School Competitive Basketball Season on Dynamic Postural Control. J Sport Rehabil. 2015 Aug;24(3):252-60.
- Hals TM, Sitler MR, Mattacola CG. Effect of a semi-rigid ankle stabilizer on performance in persons with functional ankle instability. J Orthop Sports Phys Ther. 2000 Sep;30(9):552-6.
- Janssen KW, van Mechelen W, Verhagen EA. Bracing superior to neuromuscular training for the prevention of self-reported recurrent ankle sprains: a three-arm randomised controlled trial. Br J Sports Med. 2014 Aug;48(16):1235-9.
- Reyburn, R. J., & Powden, C. J. (2020). Dynamic Balance Measures in Healthy and Chronic Ankle Instability Participants While Wearing Ankle Braces: Systematic Review With Meta-Analysis. Journal of sport rehabilitation, 30(4): 660–667.